
Ovarian Masses - Part 6 - 2
Morphology: Putting it all Together
Morphology: Putting it all Together
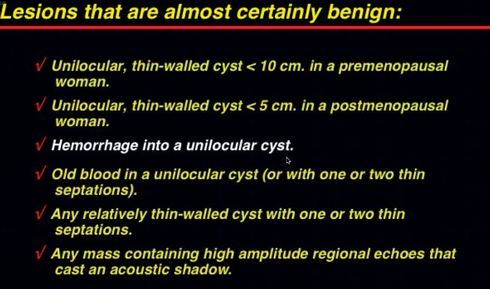
How does morphology Perform in calling something benign?
- If you think something is benign using our rules, you will be right almost every time!
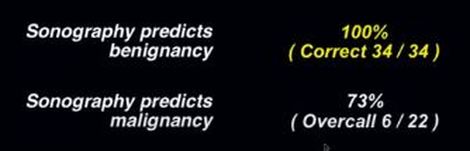
How does morphology perform when calling something malignant?
- This is where morphology struggles a bit
- In Granberg's study, ultrasound tended to overcall things malignant when they were really benign
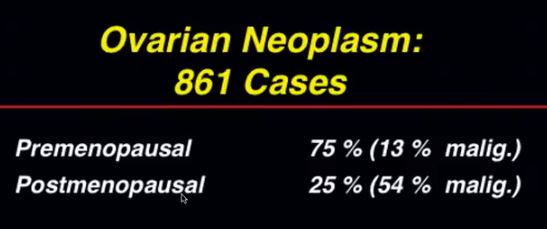
do postmenopausal women get more ovarian neoplasms?
- NO! Actually, 75% of neoplasms occur in pre-menopausal women!
- However, if you find a neoplsm in a post-menopausal woman it is more likely to be malignant
HOW GOOD IS MORPHOLOGY AT ACCURATELY DETERMINING the pathologic diagnosis OF A LESION?
- Firstly, a minority of histologic types comprise the vast majority of masses
- Benign Neoplasms
- Serous/Mucinous cystadenomas and Cystic Teratomas make up approximately 95% of all the lesions we see
- Over half are cystic teratomas and we can confidently diagnose those 75% of the time (link)
- 25% are serous cystadenomas which are either unilocular or oligoseptate, so we will confidently diagnose these as benign
- Malignant Neoplasms
- These have many types of appearances which we have already discussed, but the point is that they are NOT going to look like either a cystic teratoma or a serous cystadenoma
- Mucinous Cystadenoma (benign)
- This is the "problem child"
- These can look a lot like serous or mucinous cystadenocarcinomas
- So, again, our problem isn't calling:
- benign lesions benign or
- malignant lesions benign....
- It's calling a benign lesion malignant
So, doppler must be the answer, right?
- Watch the next video to find out!